What Is Osteopathy In The Cranial Field
Osteopathy in the Cranial Field (also called cranial-sacral therapy)
was taught by the founder of Osteopathy Dr AT Still, MD, DO and was
further developed by Dr William Garner Sutherland, D.O. (1873–1954).
Was developed as an extension to the osteopathic approach over the course of 50 years
by Dr. Sutherland who developed the key
concepts of the Cranial Approach.
The cranial concept, first put forth by W. G. Sutherland, DO and
originally alluded to by A.T. Still, MD, involves the application of
Dr. Still's principles of Osteopathy to the head (cranium) and to
the tailbone (sacrum). It is based on The Five Components of the
Primary Respiratory Mechanism.
The "cranial osteopath" is not preferential to the cranium or the
sacrum. Instead he or she includes these areas in an overall
evaluation and treatment plan, considering the whole body as one
dynamic, integrated unit of function.
It has become a specialized technique based on the belief that the tissues
surrounding the brain and spinal cord undergo a rhythmic pulsation.
This “cranial rhythm” is supposed to cause subtle movements of the
bones of the skull.
The Clinical Practitioner of Osteopathy in the Cranial Field or Cranial-sacral
Therapy should
be able to detect these rhythms and gently manipulate the bones in
time with it.
The application of
Treatments aim at:
1. Relaxing Nervous Tension
2. Equalizing Rhythm of the Cerebrospinal Fluid
3. Equalizing Circulation of the Blood Flow
4. Equalizing Circulation of the Lymph Flow
5. Transfer of Body Energy (heat and vibration)
The application of which are aim at making a positive impact on the
Anatomical and Physiological workings of the Body.
Osteopathy in
the Cranial Field
William Garner
Sutherland DO (1873-1954) graduated from the American School of
Osteopathy (ASO) in 1900. As a student of Dr. Andrew Still, he took
the admonition to "keep digging" very seriously. As a senior student
at ASO, Dr. Sutherland happened upon a disarticulated skull in the
North Hall, noting the beveled artiulcatons of the spheno-squamous
suture. He had an inspiration that the bony cranium was capable of
respiratory motion.
"Beveled...
like the gills of a fish... indicating articular mobility... for a
respiratory mechanism."
This "guiding thought"
was initially quite confusing, but Dr. Sutherland could not let the
idea go. Throughout his years of practice, with diligent research
and study, he gradually developed a revolutionary expansion of the
osteopathic concept.
Dr. Sutherland's first
public announcement of his new cranial ideas were presented in
September 1929, before a district meeting of the Minnesota
Osteopathic Association, in a paper titled "Bedside Technique" by
Blunt Bones Bill.
Dr. Sutherland called
his discovery "Osteopathy In The Cranial Field" (OCF), implying that
he did not create anything new. He had simply applied osteopathic
thinking and principles to the cranium.
With experience,
research, and a deepening of his understanding Dr. Sutherlands
concept of the cranial mechanism matured. At the core of this new
understanding lies the concept of PRIMARY RESPIRATION.
The definition of the
Primary Respiratory Mechanism (PRM):
1.
Primary: it is a system that comes "first." It underlies all
of life's processes and gives dynamism, form, and substance to all
of anatomy and physiology.
2.
Respiratory: It is the spark that gives rise to the breath,
as it moves through the tissues. It is the foundation of metabolism.
It has both an inhalation and exhalation phase.
3.
Mechanism: It is a system composed of many parts that work
together to create a whole, greater than the sum of the parts.
The beauty of Primary
Respiration is the ability to experience it directly. It is not
simply a sublime concept. In the hands of a skilled practitioner,
one connects directly with Primary Respiration to bring about a
therapeutic response. It is the guiding principle; it is the
inherent intelligence within.
Five Components of
The Primary Respiratory Mechanism (PRM)
The Primary
Respiratory Mechanism has classically been described as consisting
of fIve components. These phenomena are expressions of involuntary
physicologic motion within the central nervous system and it's
adjacent anatomy.
Each component of the
Primary Respiratory Mechanism, however, exists only in its
relationship to the function of the whole. In truth, Primary
Respiration expresses itself through all of the body, and the whole
of nature. It might be said that this intrinsic motion is a
fundamental expresion of life itself. Like most naturally occurring
phenomenon, it is only the human mind that reduces the pieces for
observation and study.
Each phenonemon is
briefly described below:
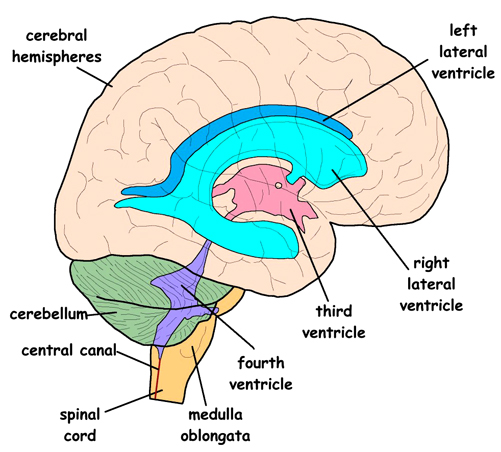
The Inherent Motility
of the Brain and Spinal Chord
The brain and spinal
cord undulate rhythmically like a jelly fish. As the brain coils and
uncoils, the cavities within the brain (ventricles) and around the
brain (cisterns) change shape. During the inhalation phase (flexion)
the brain (and bony cranium) gets shorter and wider. During the
exhalation phase (extension) the brain (and bony cranium) gets
taller and narrower.
The Fluctuation of
the Cerebro-Spinal Fluid (CSF)
It is well established
that the cerebro-spinal fluid (surrounding the brain and spinal
chord and filling the ventricles) fluctuates rhythmically. This
rhythmic fluctuation can be visually observed (and pressure changes
measured) during a typical spinal tap, and has been documented by
numerous research studies.
A controversial idea
unique to Osteopathy describes CSF movement throughout the body,
passing along the spinal nerve sheaths and through extra-cranial
lymphatics. Though initially controversial, this component of the
osteopathic concept is now being strongly supported by recent neuro-science
research.
The CSF is considered
to play a very potent nutritive role for all the tissues of the
body. In his later years, Dr. Sutherland was so impressed with the
potency of CSF, he would refer to it as "Liquid Light."
The Dynamic Shifting
of Tensions in the Dura Mater
The Meninges are the
membranes that surround the brain and spinal chord, and contain the
cerebro-spinal fluid. The Dura Mater is the toughest and most outer
layer of the meninges. The Dura Mater also has an internal
architecture comprised of 3 sickles.One runs back to front (called
the falx cerebri) and separates the two cerebral hemispheres. There
are two other sickles, one on each side of the falx (called the
tentorium cerebelli) that also run from the back to the front,
somewhat parallel to the floor (when you are standing straight). The
tentorium cerebelli gets its name from being "tent" shaped. The dura
covering the outside of the brain then attaches firmly to the
foramen magnum and upper cervical vertebrae, surrounds the spinal
cord and descends to attach to the sacrum at the 2nd sacral segment.

The "Tent" and "Falx" (brain cut away)
These dural membranes
are under constant tension. They are taut. Because of the tension
through them, we refer to the Dura Mater as a Reciprocal Tension
Membrane (RTM). If you pull on one end of the membrane, that pull is
transmitted throughout. The Dura maintains the structural integrity
of the bony cranium (as it attaches into the bones). Movement of the
brain, and CSF becomes translated into the membranes as a dynamic
shifting of the reciprocal tension.
So when the head is
traumatized, the dural membranes may become twisted and compressed.
The fulcrum around which the rhythmic movement is organized...
becomes deranged. Often these membranes are the primary seat of the
cranial dysfunction, actively distorting the bones they support.
The Articular
Mobility of the Cranial Bones
There are 22 bones in
the cranium (not including the mandible or ossicles of the ear).
They meet at the suture lines. These bones form in membrane and
cartilage. At birth the bones are not fully formed and are in fact
quite far apart from one another. As the infant is squeezed through
the birth canal, the bones slide over one another and re-expand
afterwards to resume their normal positions. This physiologic
compressibility allows for maximum brain capacity and minimizes
brain damage. All during fetal development and after birth, the
brain is constantly undulating and CSF is constantly fluctuating.
This movement is transmitted through the membranes out to the bones.
As the bones gradually grow to approximate one another they remain
in constant motion. This movement keeps the sutures patent (open).
The sutures contain blood vessels, nerve fibers, and connective
tissue, just like any joint. The amount of movement is very tiny,
100ths of an inch.
This movement of the
cranial bones is considered controversial. Conventional thinking
considers the skull to be fused. The concept of a fused skull is
erroneous, dating back to a paper written in 1873, known as "The
Monro-Kellie Doctrine." The research supporting this doctrine is
over 100 years old and was not very precise. More recent research
supports our clinical observations of cranial bone mobility.
Gradually, the mobility of the cranial bones is becoming a more
widely accepted concept.
It has been found in
some anatomic specimens that certain cranial sutures have fused.
When fusion occurs, however, it is a pathological condition. Sutural
fusion occurs because the cranium has received an impact causing the
bones to compress, and lose their sutural mobility. When any
joint in the body becomes immobile, it will fuse. (Put your arm in a
sling, and after some time you'll lose motion in your shoulder). In
health, the Cranial Sutures are patent and allow for a slight amount
of motion.
Another wrinkle... We
consider the bones themselves to actually be a very dense fluid.
They are living tissue. They are constantly being reabsorbed and
recreated. They have inherent flexibilty. Traumatic influences not
only compress bones together, but cause them to "stiffen" and lose
their fluid nature.
The Respiratory
Motion of the Sacrum Between the Illia
The sacrum is
connected to the cranium via the dural membranes that surround the
spinal chord. The dura between the occiput and sacrum is referred to
as "the core link." Attached only at the base of the skull and the
sacrum at the 2nd sacral segment, the motion of the occiput is
transmitted freely to the sacrum. The relationship of the sacrum
with the occiput becomes clinically relevant when the cause of
headaches may be due to a fall on the tailbone many years
previously.
Dr. Sutherland was the
first to discover and reason the activity of
these well known anatomic structures. This model of physiologic
activity provides an introduction to the "therapeutic process," and
an introduction to the experience of Primary Respiration.
A skilled Osteopath is
able to perceive and work with any part of this physiologic
mechanism. As incredible as this may seem, we feel the bones move,
the membranes pull, the fluids fluctuate, and even the brain
undulate. During treatment each Osteopath may find their focus to
settle upon a different aspect of this PRM. Some Osteopaths
naturally engage or are more comfortable with the bones, some with
membranes, some with fluid.
As I sit with my hands
upon the patient, I learn how trauma has established itself in the
whole person. Then as needed, I move into bone, membrane, fluid, or
potency...